
I remember when applying for IR fellowship back in 2016. The benchmark for a “good fellowship” seemed to be measured in the number of TIPS performed by the IR department each year. Oh yeah bro, I’ve done over 25 TIPS so far. Always fun to hear the IR fellow at any given program tell you how sweet their training has been. This is of course hilarious in retrospect seeing as most IRs in practice aren’t doing many TIPS.
With that being said, the blessing and curse of hospital life is you never know when you’ll be called for a portal hypertension consult. Your GI doc can potentially be in a tough spot and you may just have to slam a TIPS to save a life. In fact I had one where week where I had to do this twice.
Now you can imagine as infrequent as a TIPS procedure can be in most community settings, reducing a TIPS is even more rare. Of course as luck has it I was recently consulted on a patient with hepatic encephalopathy several months after a TIPS. Despite pretty aggressive medical management it was clear that this was a problem so I made the decision to proceed with a reduction.
I want to share with you a pretty straightforward way of doing this. First of all, credit where credit is due. The IR group at Mt. Sinai published a nice summary of this technique in 2016.
There have been some interesting ways to do a TIPS reduction including the use of parallel stents. I’ve never partook in such shenanigans. I love this sheath control technique because it so simple. Single wire. Single stent. The more IR you do, the more you realize simple is always better.
This technique involves the deployment of a balloon expandable stent-graft within the covered portion of the Viatorr stent. The stent is to be deployed such that it takes on an “hour glass” configuration.
Here’s what you need to do to get this done:
Take a balloon expandable stent graft, most commonly either an Atrium iCast or Gore VBX. 9 x 59 mm works very well.
- Line up the distal/portal aspect of the stent graft at the junction of the covered/uncovered portion of the Viatorr.
- Position the 10 Fr TIPS sheath 2 cm from the distal/portal end of the undeployed stent graft.
- Inflate your stent graft balloon to nominal.
- With the sheath still constraining the majority of the deployed stent graft, exchange out for a 12 mm x 4 cm balloon and re-inflate the distal aspect of the stent graft with the majority of the balloon again being constrained within the sheath.
- Leaving the sheath where it is, deflate the balloon and retract it to the proximal/hepatic venous end of the stent graft, 2 cm from the edge. Retract the sheath proximally and inflate the balloon to flare the proximal end of the stent.
- Now deflate the balloon and advance a 5 mm x 4 cm balloon into the central aspect of the newly deployed stent graft. Dilate to nominal
- Contrast injection from the main portal vein and measurement of pressures to see how you did.
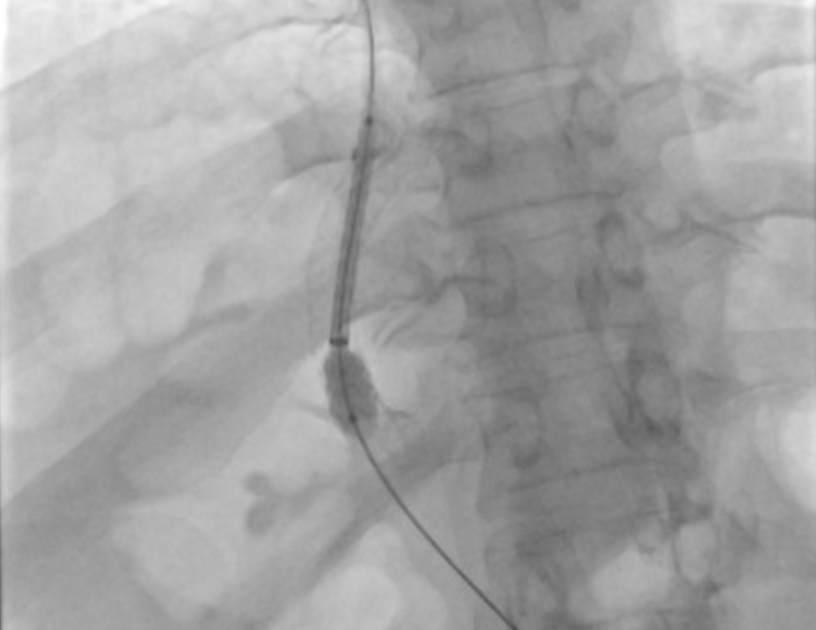
Here are some pictures from a recent case:


Have a good way of reducing a TIPS? Please share below. Always looking to learn new tricks.
Excellent result.
Thanks!