
I’ve always been a fan of alternative access. I think this probably stems from my experience in residency consistently failing to deploy a Starclose in just about every groin I touched. I still have painful memories of holding pressure while feeling just downright defeated. It turns out in retrospect that I’m totally fine at closing groins, just not with the Starclose. My apologies to Starclose users out there. Closure devices are a very personal thing. Nevertheless, it was around this time where radial access was becoming hot and the folks out of Mt. Sinai were spreading the gospel. I caught wind of the action and dove deep into this potential to not have a failed closure device! I so much as gave a talk to the entire IR division about radial access as a fourth year resident. Not claiming responsibility for a culture shift, but I do know that one talk helped move the needle in that particular department which now performs radial access somewhat routinely. Especially funny considering I gave that talk with 0 experience with radial access. Thankfully the presentation of compelling data overcame my lack of experience.
Naturally, I found pedal access very interesting as I wanted a safe way to treat my incredibly large CLI patients. I learned about pedal access from visiting Dr. Jim Melton in OKC as a first year attending. My local Abbott rep in NC flew me out there and we had a great day watching him handle CLI cases from primary pedal access including placement of an iliac stent via the foot. Simply incredible. I took that knowledge and worked on my pedal skills in the hospital, then stepped it up a notch with a sharp increase in CLI cases as I entered the OBL space.
I’ve discussed some aspects of pedal access in prior posts, but I want to focus specifically on a couple tips I’ve learned to obtain reliable access and to also discuss relevant equipment.
One question that is often asked regarding retrograde tibiopedal access is where on the foot/ankle should the vessels be accessed? The simple answer is it’s safe to access anywhere on the foot/ankle where the artery is compressible. Practically speaking, you want to access the distal AT above the tibiotalar joint which allows for more convenient sheath placement as opposed to DP access which leaves your sheath annoyingly oriented with your wires bumping against the distal foot/toes. For PT access, you have a small room of compressibility generally at the level of the medial malleolus.
When getting access, it’s helpful to be generous with lidocaine to give yourself some buffer room to track your needle safely into the vessel. Using a pediatric/hockeystick probe will make your life much easier.
When obtaining pedal access you will often get return of blood from your needle before the entire needle bevel is fully within the vessel. This means it’s entirely possible for you to pass your wire into the needle and feel significant resistance. One thing that helps in this situation is to simply flatten the needle. I find entering the vessel at a 30 degree angle (similar to radial access) makes a big difference. Another trick you can do is take a V18 wire and put the tiniest bend at the tip of the wire. You’ll notice that the wire will immediately take into the vessel and allow you to move forward with placing a sheath. This tip credit goes to Dr. Bill Julien.
With respect to sheaths, most operators I know use radial sheaths for pedal access. I’m not sure if this is just a biased sample, but I see a lot of people putting Terumo Glidslender sheaths in the tibial arteries. While it’s totally fine to do so, these sheaths are rather flimsy and are prone to kinking. Don’t get me wrong, I love using the Glideslender in the wrist because they are relatively atraumatic, but when working around the ankle, it helps to have a little more body to your sheath to facilitate insertion. Also helps to save some money too when you can. I love Terumo products, but they are expensive.
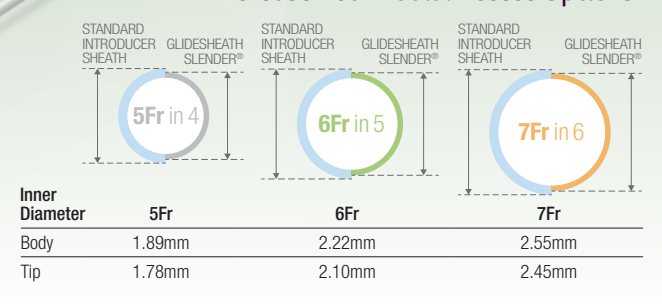
Unlike Terumo Glideslenders, Merit Prelude Ideal sheaths are categorized true to their outer diameter (i.e. a 5 Fr is a 5 Fr versus a 5 slender which is really the OD of a 4 Fr sheath with super thin walls which can accommodate a 5 Fr device). Despite this distinction, the Prelude Ideal sheaths are still relatively thin walled with average OD of only 0.2 mm larger than a Glideslender. Here are two graphics for comparison:

Measuring the vessel prior to access is incredibly important. I think in many cases, you’d be fine putting a Prelude Ideal sheath in a tibial vessel. With that being said, there are exceptions. One particular exception are older females who tend to have very small pedal vessels. In those situations the decreased diameter of a Glideslender may be advantageous, particularly if it’s the difference between being able to deliver 6 Fr devices for SFA/popliteal intervention versus sticking the groin.
After obtaining access, it is extremely important to heparinize. I have always given 100 units/kg immediately after the wire is confirmed intraluminal on ultrasound. After waiting for a minute or two, I then place the sheath. I think it’s important to check ACTs periodically with the goal of >250. Not all labs have this capability, but if you can push for it particularly early in your experience I do believe it truly adds value and keeps you out of trouble.
Prior to sheath removal, I like to give some nitro through the sheath and have a technologist hold gentle manual compression for hemostasis. Using a hemostasis band is fine too. Putting a touch of nitro paste adjacent to the puncture site can help promote patency. I always confirm distal vessel patency with ultrasound prior to leaving the room. Recovery after hemostasis is 45 minutes. Truly a beautiful thing! It is not unusual for high volume outpatient CLI operators to do 5 or 6 of these cases in a given day. Can you imagine doing that in a hospital? Good luck!
If you have tips/tricks regarding pedal access you’d like to share, please share them below. Again, I have no conflicts of interest with device manufacturers. I’m sure there are other products out there that work well.