
Seeing all the engagement on X regarding The IR Exodus was great. I had a lovely comment from an interventional radiologist 6 years out of training who has decided to go back and pursue a DR fellowship. This reader raised some interesting points and had some good questions I thought I would address here on the blog. Check out the screenshot of the comment below:
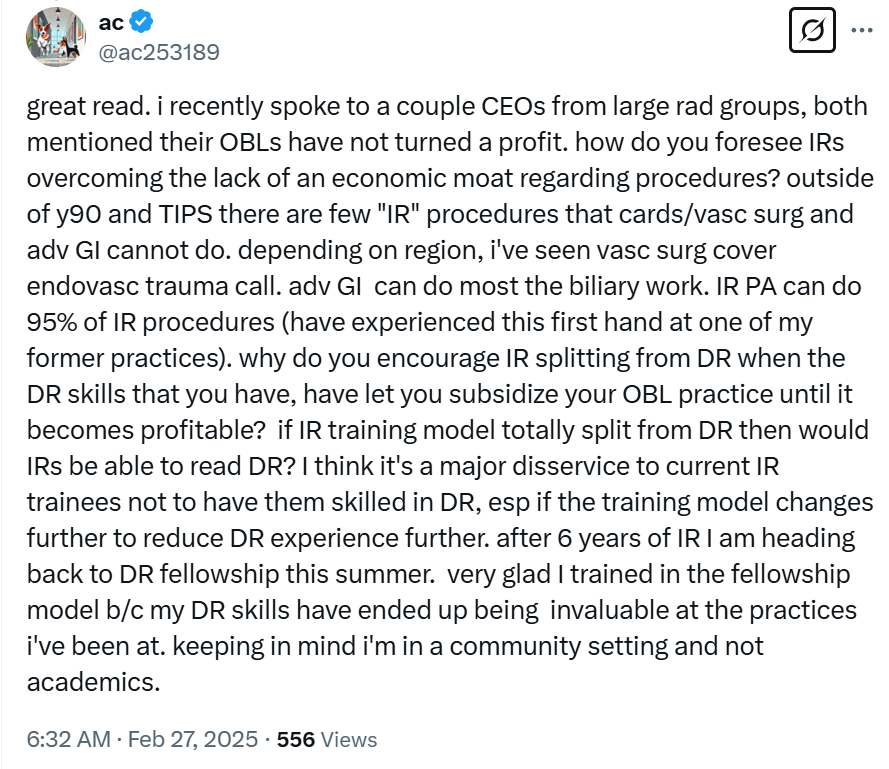
This reader asks: Why do you encourage IR splitting from DR when the DR skills that you have let you subsidize your OBL practice until it becomes profitable?
Specific to me, if I could not read DR, I would probably pick up more local IR shifts at the University of Missouri if they’d be kind enough to let me. Doing more daytime hospital-based IR would probably result in some challenges for my practice since daytime continuity is essential, and taking weekdays off when running a longitudinal clinic is hard. I could withstand up to two years of not having any outside income to support my business expenses. I should add that 95% of those savings came from doing interventional radiology on a locum basis over the last three years. If I blew through those savings, I could dip into investment funds (bad idea) or beg my academic vascular surgeon wife to fund my endeavors (also a bad idea). I’d have to go through each of these steps before I ever considered taking a loan, and you can see that none of these options involve diagnostic radiology.
If I can stay cash-flow positive, fiscally conservative, debt-averse, and spreadsheet-oriented, that option makes the most sense. That is why I do teleradiology. It is a very flexible way to fund my business without traveling and shutting down my clinic, which is problematic. However, it is by no means mandatory. Most folks who start OBLs take out huge loans.
The problem with being board-certified in DR is a global issue, with my current situation simply being a symptom of a curable disease. One particular tweet highlighted that issue right here:
Dr. Azad hit the nail on the head when he stated that IR often feels more like a hobby than a primary job for a radiologist. He is not wrong because that is precisely how it is treated in most community settings, where most of us practice. As highlighted many times on this blog, the simple economics of most hospital-based IR practices are such that professional fees alone do not cover the average salary of interventional radiologists, which are often indexed to diagnostic radiology. IR becomes an anchor for a group to secure a lucrative healthcare system imaging contract.
The simple truth is that interventional radiologists do not need to take their profession as seriously as cardiologists, vascular surgeons, or other surgical subspecialists because they directly or indirectly derive their income from an entirely different income stream in diagnostic imaging. Ceding turf in vascular was functionally of little consequence from a business standpoint. The same will apply to embolization and any other treatments that innovative IRs develop in the future.
Clinics are not as crucial for our specialty because we don’t require efficient and busy clinics to generate cases to support our incomes. That complex and undervalued work is unnecessary when reading diagnostic imaging between cases, which is far more financially efficient.
Ultimately, our field has not adopted a surgical practice pattern. If your interventional work cannot fully support your expenses and expected compensation, you have not taken your IR practice as seriously as you should. I suspect this is the case for over 90% of interventional radiologists because we do not need interventional radiology to pay our bills when working within radiology departments with a simple but effective business model focused on imaging interpretation.
If your interventional work cannot fully support your expenses and expected compensation, you have not taken your IR practice as seriously as you should.
Dependence on diagnostic radiology has hurt us in various ways. Culturally, we continue to focus our efforts on attracting individuals who are interested in radiology and less so primarily on a surgical practice pattern. It’s time for a cultural shift reflecting our value and potential, which is long overdue and necessary for survival.
However, moving beyond the critical cultural issues and keeping the current discussion focused on financial matters, it is hard to ignore how our dependence on diagnostic radiology has hurt us. Consider basic financial metrics and how the CMS Relative Utilization Committee values our procedures. This interventional radiologist summarizes this nicely in a recent IR Docs Only Facebook post, highlighting the stark financial challenges we face:
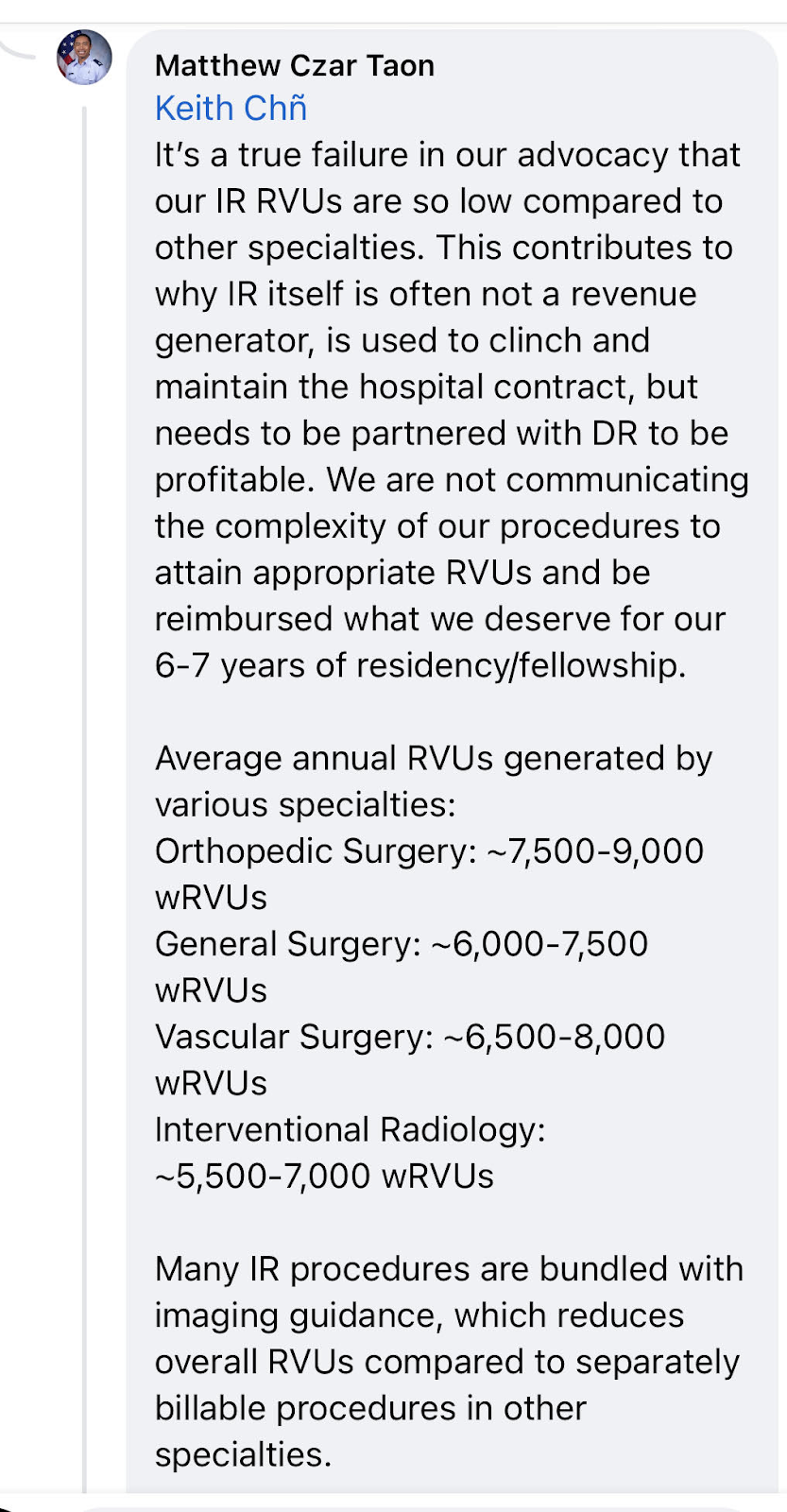
The fact that radiologists are “productive” from a wRVU standpoint means our procedures have been relatively devalued compared to surgical procedures. We have done a poor job advocating for ourselves, probably because this has been unnecessary because of our relationship with diagnostic radiology.
The reader is correct that we do not have many “IR-specific procedures,” but we cannot survive without competing with other specialists. We are not the only specialty with turf battles. We continue to cede turf because we fail to adopt a surgical practice pattern, which is ultimately related to the fact that we don’t need to adopt it to make a living.
So, ultimately, the only way to take ourselves seriously is to cut the diagnostic imaging cord altogether. Until we do that, we will continue to devalue our work, treat IR as a hobby, and live in a world where most IR physicians must maintain diagnostic radiology skills to make a living. This will not end unless our professional society pushes for a fundamental change in our board certification. It is not a popular move, but saving our actively dying specialty is necessary. As a community, we can advocate for this change and save our specialty from extinction.
If we were serious about being surgeons, we would not have trained as radiologists in the first place. The field exists for the ‘surgery curious’ ; one who wants to hold a knife but not spend their life in the hospital. The professional + karmic results are pretty much spot on. A ‘real surgeon’ would never contemplate spending 4 yrs of their life behind a computer screen
A couple things. You and I trained in different times compared to the younger IRs today. Now they spend 3 years behind a computer screen. We have a unique group within our larger specialty that enjoys a surgical practice pattern and performing interventions which are derived from their clinical endeavors and not from imaging findings alone. For us, imaging is one of several tools that we use to take care of patients. This unique field of medicine operates from head to toe in a minimally invasive fashion. We add tremendous value in the treatment of common conditions that affect over 50 million American and over a billion people globally. To simply not see this but to reduce our existence to radiology versus surgery is frankly reductive, regressive, and ignorant of this new physician phenotype that is evolving before our very eyes.
Exactly. The field is too new, early in its evolution. I would have liked to enter it in its old glory days, after all the kinks had been worked out. “Dr Gaur, your 3-level kyphoplasty is on the table”. “Dr Gaur, your TIPS patient just cartwheeled thru the hallway”. “Dr Gaur, your driver is waiting for you in a purple Rolls Royce”. Wake me up…
Thank you for the post ! As a DR trainee with a significant interest in IR , do you see ESIR and Independent IR residencies going anywhere in the near future ?
I don’t think so. I think academic leaders want to continue to train as many “IRs” as humanly possible and will leave all options open.
Not all IRs are built the same. I think most who are trained in IR end up practicing some version of “IR lite” and in reality there are maybe 50 or so graduates a year who end up being committed to a surgical practice pattern. I think the integrated pathway is a better way (albeit still very flawed) for those who want to focus on a surgical practice pattern as an attending.
I believe integrated is a good path at only a few select programs dedicated to clinical ir. Too many integrated programs are just looking for free labor to cover calls and inpatient lines and tubes biopsies, and in that case better to do Dr esir and have a chance at going to the top clinical fellowship
Good point. Thanks for commenting.
The training programs are too varied.
Some have limited clinic and admissions.
Some do PAD some do not. Some have a lot of critical care training some do not. Some do pain and spine some do not. Some do PE and DVT and some do not. Most do cancer work and lines and drainage procedures. The variability in training is a big challenge. We need to do a better job in standardizing training.
I agree completely. Thanks for your comment.
From a medical student who will apply to IR residency match in less than a year, every time I hear the word “ceding turf to vascular”, my blood boils. I don’t want to do that (ceding turf to a procedure I’d want to offer in the future), it makes me want to outwork every-single vascular surgeon out there, hold clinics, have extra-ordinary cases that pays me just like how it would pay a surgeon. It’s nonsense to me that an IR practice can’t be profitable, because that’s like saying a surgical practice can’t be profitable. I may be surgically inclined, but I don’t like cutting people open. Not because I can’t, because I think the future of medicine is percutaneous, endovascular, minimally-invasive and targeted. Do you think if there was an IR way to treating pancreatic cancer, would people be open to getting Whipple procedure? Of course not! Hence, if the powers that be want me to study 3 years of diagnostic imaging, I’ll do that to get there, and have another skillset under my belt, no issues with that, but I’ll be 100% IR. I’ll be the best for my patients, so that my colleagues will have no concerns referring their patients to me over a run-of-the-mill vascular surgeon, or interventional cardiologist. As a future trainee, I’ll do whatever I have to do get there, then I’ll advocate for things to get better for the generation after mine. One thing for sure, we need to define what it means to be an interventional radiologist, set professional expectations for our primary care/hospitalist colleagues, and disseminate this information as best as we can. We need to put it on billboards if need be.
This is the energy we need.