
I recently received a question from a reader. I decided to post this question for you all to see, deidentified, of course, to protect the trainee asking this, in an effort to share what I have learned regarding finances as an IR attending. For context, I am now in my eighth year since training and am speaking from the lens of someone who owns and operates a small outpatient practice.
Hi, I hope you’re doing well! I am an intern who has matched into IR.
I’ve been having a lot of second thoughts and doubts. I feel like SIR paints the field in a very different way from how it is actually practiced. I’ve also read a lot of your posts online- one that really stuck out to me was when you said you would not pick this field again if you had to choose again.
I definitely like the idea of doing high-end IR (dealing with bleeds, potential to do neuro IR, interventional oncology, TIPS, etc.), but 1) I’m not enamored with the bread and butter (lines, tubes, drains), and 2. I do have a lot of business interests and would like to do private practice. From my understanding, you can’t really do a lot of the advanced procedures in private practice and OBLs are pretty few and far between right now as the field is still in its infancy in a lot of ways.
I have been considering switching to internal medicine and then pursuing a GI or interventional cardiology fellowship. I would get to do procedures, which is what I want. There’s also quite a bit of interest in those fields in business and in increasing income. This is one of my main concerns if I am being brutally honest.
That is my main question for you as well as any advice you can offer- do GI and cardiology tend to make substantially more than IR? Based on MGMA data, it would appear not, but I know that data does not tell the full story. I’ve also read about your struggles with starting your own OBL- are OBLs common enough that I could just join one (as you can with GI and cardiology groups) or would my concerns just be better addressed by switching? I’d love to hear any thoughts you might have!
Sincerely,
Concered Intern
Dear Concerned Intern,
I am glad you asked this question. Unfortunately, financial matters in medicine are very taboo. From our days in medical school, we are conditioned not to discuss economic issues openly. The situation is further strained by the fact that our mentors in medical school and residency are often employed academic physicians who may not have a clear understanding of how dollars flow in American healthcare. They teach, research, and treat patients, and leave the money to others. As such, we in turn put our heads down, work hard, but inside have a good sense of which pathways will yield a financial reward because let’s not lie about the fact that we devote over 14 years of post-high-school education to get to our first job at age 32 after taking out over $300,000 in student loans.
Healthcare in the US is a very convoluted industry that is, frankly, full of waste. Our country spends over four trillion dollars a year on healthcare, which amounts to more than 20% of GDP. Less than 8% of this actually goes towards physician pay.
The one thing every student or pre-med reading this blog needs to understand is that, despite being a beacon of free market enterprise for the world, American healthcare is anything but a free market. In fact, it is entirely dictated by the US government. In particular, payment for services is benchmarked by the government, including what we as physicians make in the “fee-for-service” model, which drives the current healthcare landscape.
Our payment is often explicitly derived from something called the “Medicare Physician Fee Schedule.” This is basically a list of different services (CPT Codes) with a dollar amount assigned to each. To go even deeper, each service is assigned a “Relative Value Unit” (RVU) that reflects its value. Specifically, a group of physicians from all medical specialties convene as a committee, known as the AMA RVS Updated Committee (RUC) to assign RVU numbers to each service and for any new services. The catch is that the committee must adhere to budget-neutrality constraints. So, in other words, if a service has an increase in RVU, another service will have to be cut.
Please excuse my brevity, as the above process really needs a blog post or video tutorial in its own to do it justice; I’m just presenting the highlights to get my point across. Just know that over time, the amount of dollars per RVU (something called the “Conversion Factor”) has been decreasing, particularly with respect to inflation.
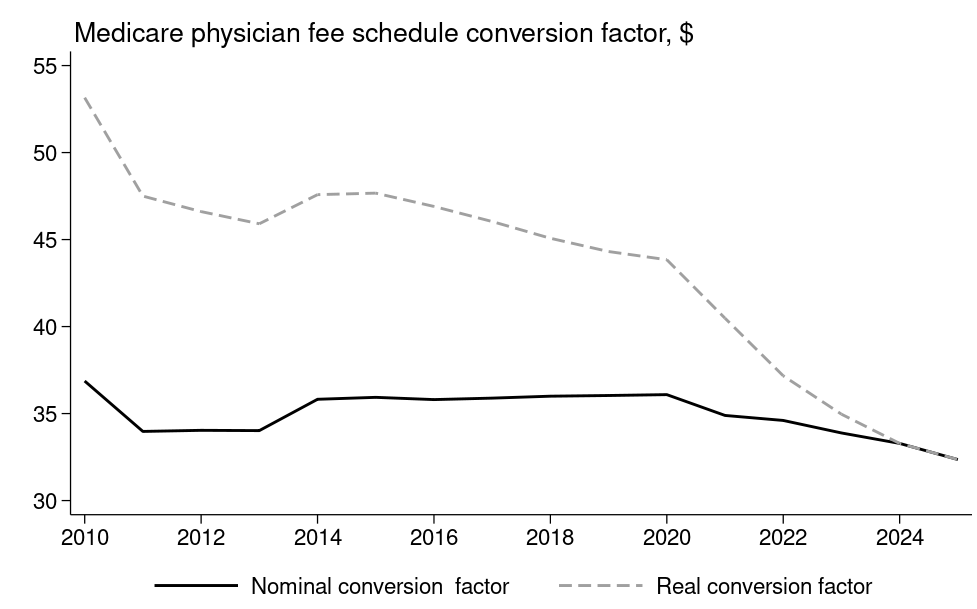
It’s easy to feel very depressed when looking at the chart above. Over time physician pay has remained relatively flat to decreasing, but when you compare it to inflation (real conversion factor) we have suffered massive cuts over time.
The situation has been even more profound for many medical subspecialists, including diagnostic and interventional radiology as our procedures have been devalued over time.

Despite the cuts, radiology, as a whole, has been very well-positioned in the American healthcare system as a lucrative specialty. Interventional radiology, for all intents and purposes, has been historically viewed as a mere appendage to radiology, so when it comes to salary trends, think about IR in the same bucket as DR (more on this in a bit).
When looking at radiology salaries over time, they have actually been somewhat increasing. The figures below are a bit outdated, but the average compensation now is closer to $700,000.

How could radiologists have rising salaries when we have had such significant reimbursement cuts over time?
There are three main factors:
1. Demand For Imaging Services
There has never been a greater demand for imaging than the present. I do not know of a single radiologist who has been experiencing a decreasing list. Furthermore, as more advanced practice providers care for patients, the demand for imaging is increasing. I will say anecdotally, having interacted with trainees now and comparing it to my experience as a diagnostic resident from 2013-2017, volume has significantly grown, and it’s not unusual for trainees to read over 60 cross-sectional studies on a night shift.
2. Technological Improvements
We can read more efficiently than ever before thanks to improvements in PACS, dictation software, clinical decision-making tools, and, especially now, with AI.
3. Healthcare System Payment
As imaging services continue to grow, we are facing a severe shortage of radiologists in the market. The supply-demand imbalance has been so stark that many private practices have struggled to hire radiologists. Many groups are now asking their healthcare system clients for subsidies to remain competitive in the marketplace. So now, instead of all payments coming from the declining Medicare Physician Fee Schedule (MPFS), we are seeing physician compensation coming from another “bucket” in healthcare: payments to healthcare systems. Unlike payments to physicians, payments to facilities like hospitals are increasing over time.

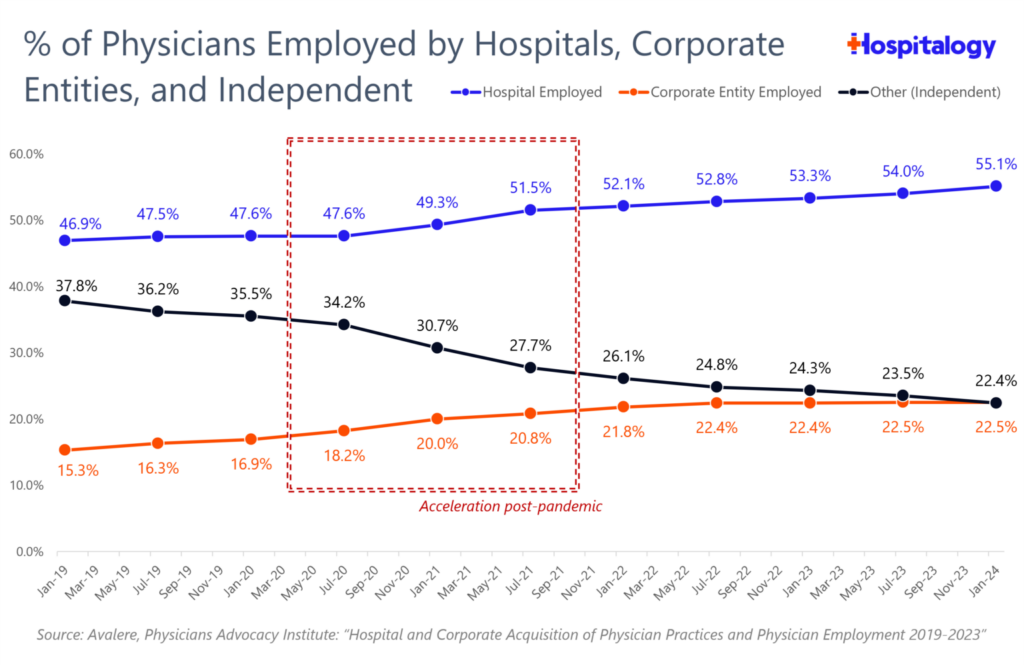
Many private practices are choosing to fold and become employed by their former healthcare system clients, or to receive buyouts from private equity firms. The “following the money” trend in medicine is very real, as reflected in the fact that the vast majority of physicians are now employees rather than owners of their medical practices. Approximately 80% of all physicians are either employed by a healthcare system or by private equity. The situation is further harmed by the fact that many younger physicians may not be interested in owning their practices due to a combination of generational attitudes towards life that differ from those of their predecessors and economic headwinds.
The reason interventional radiology salaries have increased is based on two factors:
- Most interventional radiologists are really diagnostic radiologists.
The vast majority of interventional radiologists read a lot of diagnostic imaging and derive most of their income through those reads. For many interventional radiologists, their procedures are merely a service to their healthcare system clients to maintain diagnostic contracts. This is a harsh reality that I learned in my first two years of practice. This one fact would have saved me a lot of heartache.
2. Clinical Interventional Radiologists are at best “aligned” and at worst employed by healthcare systems.
Interventional radiologists practicing in a clinical model cannot produce RVUs comparable to those of diagnostic radiologists and therefore require some form of payment outside the MPFS payment bucket to support their salaries. This money comes from healthcare systems. The very savvy who choose to remain independent can often do so by instituting a professional services agreement (PSA) with a healthcare system. This is possible and currently supported by a supply-demand imbalance. While it is admirable, I do worry about a slippery slope towards inevitable employment, as we are not immune to the rest of medicine. Many colleagues will choose employment with lower RVU thresholds and payments well above what could be supported by physician payments alone. This is the path actively promoted by our own professional society. Please note that I do not speak for the society, and the words on this blog reflect my own opinions. Still, it is clear from their economic programming that defining our field in the context of an employed model is what our leadership is actively promoting—more on this in a future post.
Physician-Owned Outpatient Practice: An Exception To The Rule
Unlike you, the very astute and intelligent intern, it took me over 2 years as an attending to learn what you have learned in the last five minutes reading this post. I hate people telling me what to do, and I didn’t spend the best years of my life sacrificing for my patients to work for some bureaucratic institution, so I decided to take matters into my own hands.
The way the rules in American healthcare work is that if you want the most freedom possible in how you care for patients and structure your professional life, you need to eliminate as many layers between you and the patients you serve. If you are accepting insurance payments, the only way to effectively do this is to own your own practice. Independent contracting with healthcare systems and physician practices is the second way to do this, though it does not afford the same practice freedoms as owning your own practice.
The challenge has been that with declining MPFS payments, rising inflation, and increasing costs of capital equipment, disposables, labor, and rent, we are being squeezed. Despite this, the shining star for IR is that what we do still pays relatively well, particularly in an office-based setting, provided you can keep your costs in check and provide a good service to keep referral streams alive.
The OBL path is the only path where one can still make a market wage or higher, practicing clinically and longitudinally, without being tied to hospital payments and the associated strings, and ride on a slippery slope to inevitable employment that could be. Even groups that provide hospital services maintain independence by having robust outpatient practices in physician-owned settings (either OBLs or Ambulatory Surgical Centers).
It is a very challenging path. I am figuring it out for myself. It’s not easy, but it’s working so far. I do not think it is a realistic path for most interventional radiologists for several reasons: lack of clinical training, leadership skills, financial competence, and risk tolerance, given an opportunity cost that is higher than it has ever been with current market wages.
So I’m not going to blow smoke up your rear and act as if you can easily do this, because you can’t. This path is literally meant for those who feel like they have no other option. Generally reserved for those with a perpetual chip on their shoulder and who are always trying to prove something. If this doesn’t summarize you, then do not take this path.
Now, by the time you come out of training, there will likely be more outpatient settings where you can take a job as an employee. I would not expect a significant salary from those positions unless you can handle a large caseload. Anyone who owns that practice and pays increasing overhead out of a declining pot of money will need you to spin faster and faster to keep those lights on.
IR, GI or Cardiology?
At the end of the day, private practice in each of these fields is in jeopardy. No matter which field you pick, you will have a very high likelihood of being employed by some hospital system. You will also have a very high probability of making somewhere between $500,000-$1,000,000 a year, working very hard for that salary. Lots of call. Lots of stress.
If you’re in IR, you will either be reading a lot of diagnostic studies or doing a lot of cases. In GI or cardiology, you will have jam-packed clinics and do a lot of the same low complexity procedures over and over to keep the RVU machine humming.
So it really does not matter from a financial perspective, because one field is unlikely to offer you a significant economic advantage over the other. Most subspecialists make between $500,000 and $1,000,000. They also pay a lot of taxes and generally do a poor job of saving. At this level of income, what you do with the money you make is more important than the actual amount. It’s probably the answer you don’t want to hear, but it is the truth.
To live a clinical life where you can exceed a high six-figure specialist salary requires ownership in your practice or a facility such as an ambulatory surgical center. It is objectively easier to do that in cardiology or GI than it is IR for a multitude of reasons: pre-existing legacy clinical fields with mature practices that have clear recognition by referring physicians inherent in their organ system-based existence, versus a field that has failed to define itself thus far and requires significant collaboration with other medical and surgical subspecialists. Additionally, interventional radiology faces structural challenges posed by pseudo-exclusive contracts, which preclude ambulatory practices in many settings. Please look up old blog posts for more details. Despite it being easier in GI or cardiology than IR, it does not translate to significantly higher pay, given the economic headwinds I described and the erosion of private practice and associated physician ownership.
So in summary, pick what you like and make the most of it. I chose IR because I like the breadth of procedures and the challenges faced when dealing with a variety of organ systems. Our field is both a blessing and a curse. My career has led me to forge a new path, and I hope others can join me in better defining what we do and cementing our place as valued independent clinical specialists. It’s not for everyone, but for the right person, it’s fantastic.